Summary
DOI: 10.1373/clinchem.2012.202283
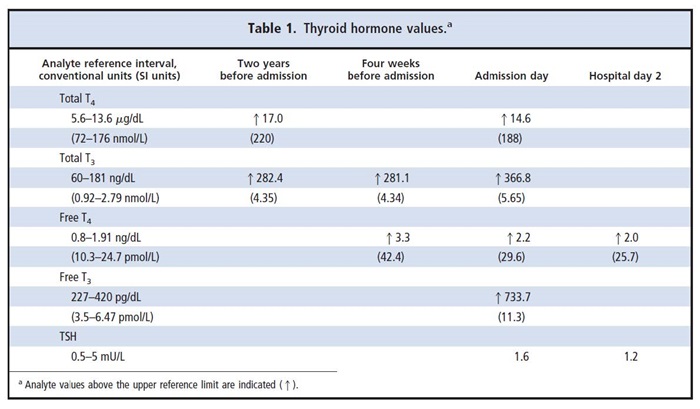
A 44-year-old Caucasian male was transferred to our hospital for increased concentrations of thyroid hormones and constitutional symptoms, including fatigue and muscle tenderness of 6 weeks' duration. Four weeks before admission, the patient's primary care physician found a diffuse goiter and ordered thyroid hormone testing (Table 1). Two weeks later, the patient developed generalized muscle pain and began a weight loss of 10 pounds until the day of admission.
Student Discussion
Student Discussion Document (pdf)
Julio Leey1* and Philip Cryer2
1 Diabetes and Endocrine Care of Alton, BJC Medical Group, Alton, IL; 2Division of Endocrinology, Metabolism and Lipid Research, Washington University School of Medicine, St. Louis, MO.
* Address correspondence to this author at: Diabetes and Endocrine Care of Alton, BJC Medical Group, 2 Memorial Dr., Suite 203, Alton, IL 62002. Fax 618-433-6179; E-mail [email protected].
Case Description
A 44-year-old Caucasian male was transferred to our hospital for increased concentrations of thyroid hormones and constitutional symptoms, including fatigue and muscle tenderness of 6 weeks’ duration. Four weeks before admission, the patient’s primary care physician found a diffuse goiter and ordered thyroid hormone testing (Table 1). Two weeks later, the patient developed generalized muscle pain and began a weight
loss of 10 pounds until the day of admission. One day before admission, he had fever and diarrhea. The patient was then transferred with the suspicion of severe hyperthyroidism.
The patient’s medical history included “hyperthyroidism” and goiter diagnosed at age 24 years. Since then, he has intermittently taken propylthiouracil several times for short periods. At age 34 years, the patient experienced anxiety, tachycardia, and spells of muscle pain. He underwent radioiodine therapy at that time but experienced no improvement in the symptoms or goiter. A few months later, the patient underwent a
repeat radioactive iodine treatment with the same unsuccessful result. He has experienced anxiety and tachycardia spells, which were intermittently treated with propylthiouracil for short periods with no relief. He also experiences chronic cluster migraine headaches.
At admission, the patient’s vital signs were as follows: temperature, 37 °C; pulse, 94/min; blood pressure, 140/70 mmHg. There was a diffuse goiter, with the thyroid gland approximately 4 times normal size. The patient had no eye bulging, eyelid lag, tremor, or brisk reflexes. His skin texture was normal. The following day, his pulse was 80/min, and his blood pressure was 120/70 mmHg. The patient’s fever and diarrhea had resolved, and he remained afebrile.
An investigation of the discordant results in thyroid function tests was initiated.
Questions to Consider
- List some causes of goiter, increased free T4 and free T3 values, and a normal TSH result.
- What laboratory tests could be done to help determine the cause of these laboratory values?
- What is the role of clinical findings in confirming the diagnosis?
- Is there a molecular test that can help to confirm the diagnosis?
Final Publication and Comments
The final published version with discussion and comments from the experts appears
in the December 2013 issue of Clinical Chemistry, approximately 3-4 weeks after the Student Discussion is posted.
Educational Centers
If you are associated with an educational center and would like to receive the cases and
questions 3-4 weeks in advance of publication, please email [email protected].
AACC is pleased to allow free reproduction and distribution of this Clinical Case
Study for personal or classroom discussion use. When photocopying, please make sure
the DOI and copyright notice appear on each copy.
DOI: 10.1373/clinchem.2012.202283
Copyright © 2013 American Association for Clinical Chemistry