Summary
DOI: 10.1373/clinchem.2012.190710
Two siblings were referred for workup for progressive neurological deterioration. The elder sibling was a 16- year-old boy who had been asymptomatic until 9 years of age when he developed walking difficulty that progressed to a bed-bound state followed by regression of cognitive function and generalized tonic clonic seizures.
Student Discussion
Student Discussion Document (pdf)
David Haarburger,1* Rudi Renison,2 Surita Meldau,1 Roland Eastman,2 and George van der Watt1
1Division of Chemical Pathology, Groote Schuur and Red Cross War Memorial Children’s Hospitals, National Health Laboratories Service, University of Cape Town; 2Division of Neurology, Groote Schuur Hospital, University of Cape Town.
*C17 NHLS Laboratory, Groote Schuur Hospital, Private Bag, Observatory, 7937, South Africa. Fax 27-21-404-4105; E-mail: [email protected].
Case Description
Two siblings were referred for workup for progressive neurological deterioration. The elder sibling was a 16-year-old boy who had been asymptomatic until 9 years of age when he developed walking difficulty that progressed to a bed-bound state followed by
regression of cognitive function and generalized tonic clonic seizures. The younger sibling was a 14-year-old girl with onset of similar symptoms at the age of 6 years. The siblings were the eldest of 6 children from a family with no history of consanguinity.
Both children principally ate a high-carbohydrate (maize)-based diet with sporadic access to fresh produce and animal protein. They had reached normal developmental milestones until the onset of symptoms. Both children had been treated unsuccessfully with sodium valproate. On examination, they demonstrated minimal communication skills and severe
cognitive impairment. They had spastic paralysis of all extremities.
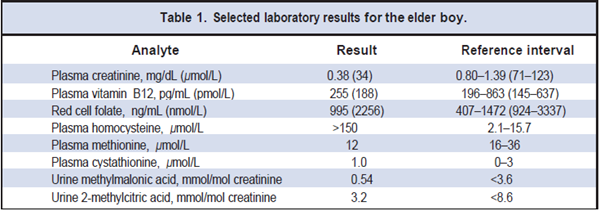
Electroencephalography in the elder sibling revealed generalized, highly potentially epileptogenic foci, and a brain computed tomography scan demonstrated marked cerebral atrophy with minimal white matter. Initial laboratory investigations, including a complete blood count, measurement of electrolytes and urea, and thyroid and liver function tests, were all within reference intervals. Syphilis serology was negative. Screening for inherited metabolic diseases included measurements of plasma amino acids and urine organic acids. Selected laboratory results of the elder boy are provided in Table 1.
Questions to Consider
- What is the most common cause of a highly increased (>50 μmol/l) homocyteine?
- Which nutrient deficiencies are associated with increased homocysteine concentrations?
- What are the deleterious effects of increased plasma homocysteine concentrations?
Final Publication and Comments
The final published version with discussion and comments from the experts appears
in the August 2013 issue of Clinical Chemistry, approximately 3-4 weeks after the Student Discussion is posted.
Educational Centers
If you are associated with an educational center and would like to receive the cases and
questions 3-4 weeks in advance of publication, please email [email protected].
AACC is pleased to allow free reproduction and distribution of this Clinical Case
Study for personal or classroom discussion use. When photocopying, please make sure
the DOI and copyright notice appear on each copy.
DOI: 10.1373/clinchem.2012.190710
Copyright © 2013 American Association for Clinical Chemistry