I took a new job as a supervisor in a medium-sized hospital lab. The lab is in reasonably good shape with no emergent problems, but my co-workers and I agree that certain areas need improvement. I am confident I can do a quality improvement (QI) project and have worked in organizations that used different approaches—like Lean, Six Sigma, and homegrown strategies—and feel I will be able to fit into any system. I know how to choose metrics and incremental goals. But how do I know which problems to work on first? It is important to me that these first QI projects succeed and are meaningful to the staff.
I am already a big fan of yours. I like that you are comfortable performing QI. More laboratorians should be confident that they can do significant QI, without learning a dictionary of jargon, without hiring an army of outside consultants, and without taking a hundred hours of classes.
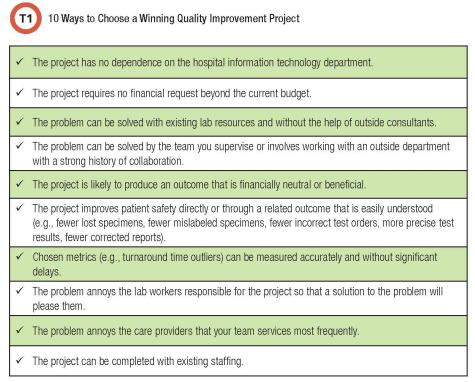
It is understandable to want early QI successes in a new supervisory job. Success in QI produces many benefits. It improves patient safety and usually is financially beneficial as well. In addition—and this is extremely underappreciated—QI is the biggest morale builder in the lab. It is better than ice cream socials, trust-building retreats, and staff appreciation lunches. This is because the overwhelming majority of lab workers come to work to do a great job. Errors ruin everyone’s day. No one likes working at a place that regularly delivers harm and poor service to patients. Creating a system in which your team regularly improves quality and feels empowered to do so will lead to highly engaged employees. Table 1 lists characteristics of a project that will produce an early win. Use this list of characteristics as a checklist to compare and contrast among potential projects.
Several good information sources are available to help you create a list of potential projects. The first and best source is the lab staff that you supervise (1). A recent CLN article explains a simple way to reveal quality problems bothering the staff: Conduct individual interviews so all staff members are heard, not just those who are particularly outspoken. Interview each person for 15–20 minutes using the same questions. A brief interview has just three questions and two are related to quality: 1) What is your job and how long have you worked here? 2) What is going well here from a quality perspective? and 3) What areas of quality worry you and could be improved? Another way to pose the last question is: What about our work worries you about potential harm to patients? Feel free to dig a little deeper on quality issues if the list of improvements is long. For long lists, ask staff to rank their suggested improvements.
The units that your team services the most—medical, surgical, intensive care, operating room, emergency department—are great sources for suggested QI projects. Care providers in these areas are a veritable wellspring of ideas and can be queried using the simple structured approach outlined above.
In addition to input from your team and the care providers they service, management reports are an excellent source of data to help create a QI project list. Focus on data-rich reports that are already available or readily obtainable without a lengthy fight with your IT department. These often include turnaround time reports, incident reports, and corrected reports. For turnaround time reports, focus on outliers, especially for tests often ordered in a critical care setting like troponin, potassium, and hematocrit. For corrected reports, emphasize corrections that changed a diagnosis or treatment. For incident reports, focus on incidents that happen the most frequently and that have affected patients.
Once you’ve collected information from lab staff, care providers, and management reports, make a list of potential projects. Use the ten items in Table 1 to compare and contrast the projects. An obvious candidate may rise to the top. If not, have your team vote on the top two projects.
The project that is chosen will likely be described with a general statement (e.g., improve speed of myocardial infarction diagnosis by decreasing average turnaround time for troponin and decreasing outliers; improve patient safety by decreasing the frequency of mislabeled specimens; improve patient safety by decreasing errors in sendout test orders; improve rheumatologic diagnosis by improving the accuracy and precision of autoantibody panels). Performing the project will require making the objective more specific, choosing appropriate metrics and interventions, and sustaining those interventions. Table 2 shows some do’s and don’ts that will help build on a general problem statement to outline a successful QI project.
I am confident you are going to choose one or two meaningful early projects and succeed. This will show your team that they are empowered to improve quality. Once a system is established for making small improvements, try more ambitious improvements like physical plant changes, major equipment changes, a major IT improvement, or adding a significant new service.
Michael Astion, MD, PhD, is clinical professor of laboratory medicine at the University of Washington department of laboratory medicine and medical director of the department of laboratories at Seattle Children’s Hospital. +Email: [email protected]
References
1. Astion ML, Messinger B, Ahlin P, et al. Collected wisdom on patient safety. Clinical Laboratory News 2010;36(7).
2. Astion M and Hernandez J. Should I stick with this turnaround or quit? Clinical Laboratory News 2017;43(7).
CLN's Patient Safety Focus is supported by ARUP Laboratories
