Summary
DOI: 10.1373/clinchem.2018.300970
A woman presented to the emergency department with abdominal pain, nausea, and vomiting.
Student Discussion
Student Discussion Document (pdf)
Ayesha Farooq, Angela Treml, and Jessica M. Colón-Franco*†
Department of Pathology, Medical College of Wisconsin, Milwaukee, WI.
*Address correspondence to this author at: Laboratory Medicine, Cleveland Clinic, 10300 Carnegie Ave., Cleveland, OH 44106. Fax 216-445-0212; e-mail [email protected]
†Current affiliation: Pathology & Laboratory Medicine Institute, Cleveland Clinic, Cleveland Ohio.
Case Description
woman presented to the emergency department with abdominal pain, nausea, and vomiting. On examination, she had abdominal tenderness and a medical history of diabetes mellitus type 1, hypertension, end-stage renal disease, liver disease (hepatic steatosis), hypothyroidism, chronic obstructive pulmonary disease, and congestive heart failure. The patient denied alcohol use or abuse.
Lipase was 680 U/L (reference interval, 13–60 U/L) and triglycerides were >4425 mg/dL [reference interval, <150 mg/dL (50 mmol/L)]. These results, along with clinical and radiologic findings, suggested a diagnosis of hypertriglyceridemia-mediated pancreatitis.
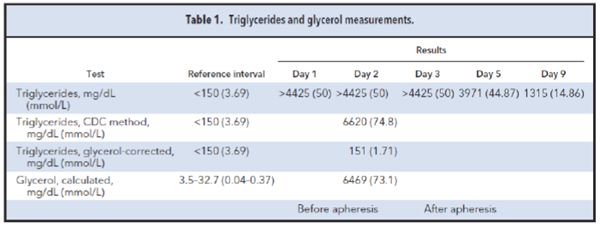
The patient was treated with insulin and heparin, but triglycerides remained >4425 mg/dL. Consequently, plasmapheresis was used to reduce the serum triglyceride concentrations on day 3 posthospital presentation, but triglycerides persisted at >4425 mg/dL (Table 1). The transfusion medicine team noticed the appearance of clear plasma during the next plasmapheresis course and called the laboratory to investigate.
Triglyceride testing in a reference laboratory followed (Table 1). The CDC method also revealed markedly increased triglycerides at 6620 mg/dL (74.8 mmol/L). However, triglycerides were 151 mg/dL (1.7 mmol/L) in a glycerol-corrected triglyceride assay (Roche Triglyceride/Glycerol Blanked Reagent, Roche Diagnostics). Glycerol concentrations were calculated (triglycerides, CDC - triglycerides, glycerol corrected) to be 6469 mg/dL (73.1 mmol/L) [reference interval, 3.5–32.7 mg/dL (0.04 – 0.37 mmol/L)]. In other words, 6469 mg/dL (73.1 mmol/L) of the 6620 mg/dL (74.8 mmol/L) in this sample represented free glycerol and not triglyceride-derived glycerol.
Questions to Consider
- What is measured in blanked and nonblanked triglyceride tests?
- What conditions could lead to these findings?
- How can the laboratory identify falsely increased triglycerides?
Final Publication and Comments
The final published version with discussion and comments from the experts appears
in the October 2019 issue of Clinical Chemistry, approximately 3-4 weeks after the Student Discussion is posted.
Educational Centers
If you are associated with an educational center and would like to receive the cases and
questions 3-4 weeks in advance of publication, please email [email protected].
AACC is pleased to allow free reproduction and distribution of this Clinical Case
Study for personal or classroom discussion use. When photocopying, please make sure
the DOI and copyright notice appear on each copy.
DOI: 10.1373/clinchem.2018.300970
Copyright © 2019 American Association for Clinical Chemistry