Summary
DOI: 10.1373/clinchem.2016.269555
A 33-year-old woman presented for the first time at the age of 9 years with recurrent seizures and was subsequently treated for epilepsy for 2 years.
Student Discussion
Student Discussion Document (pdf)
Bettina Chale-Matsau,1 Chantal van Niekerk,1 Tanja Kemp,2 and Tahir S. Pillay1,3*
1Department of Chemical Pathology, University of Pretoria and National Health Laboratory Service Tshwane Academic Division, Pretoria, South Africa; 2Division of Endocrinology, University of Pretoria, Pretoria, South Africa; 3Division of Chemical Pathology, University of Cape Town, Cape Town, South Africa.
*Address correspondence to this author at: Department of Chemical Pathology, University of Pretoria, Pretoria, South Africa 0007. Fax +27-012-328-3600; e-mail [email protected]/p>
Case Description
A 33-year-old woman presented for the first time at the age of 9 years with recurrent seizures and was subsequently treated for epilepsy for 2 years. At 11 years of age, it was noted that the patient had hypocalcemia with an increased parathyroid hormone (PTH) measured with use of an intact PTH assay. Serum calcium was 5.73 mg/dL [1.43 mmol/L; reference interval (RI) 8.82–10.42 mg/dL (2.2–2.6 mmol/L)]; serum phosphate was 10.42 mg/dL [3.36 mmol/L; RI 1.86–4.34 mg/dL (0.6 –1.4 mmol/L)]; and PTH was 319.68 pg/mL [33.9 pmol/L; RI 8.49–68.84 pg/mL (0.9 –7.3 mmol/L)]. Vitamin D (Total 25-OH; 25-OH D2 and D3) concentrations, magnesium concentrations, liver and renal function tests were all normal. No other endocrine abnormalities such as thyroid or gonadotropin resistance were detected. The patient also was of short stature and was overweight. However, she became overweight after the age of 13 years (body mass index at 13 years was 22.8
kg/m2), and the short stature was not significant, as she was at the lower end of the RI for height at 1.55 m. There was no cognitive impairment. Positive Chvostek sign was observed but not Trousseau sign.
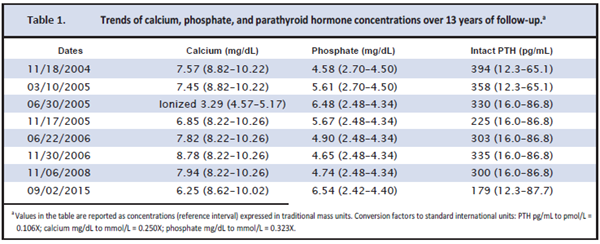
The patient was placed on active vitamin D (alfacalcidol) and calcium supplements. The patient was followed up for 13 years; selected laboratory results are presented in Table 1. Although the patient was managed on calcium supplements and active vitamin D and followed up at a tertiary endocrine clinic, serum phosphate concentrations remained persistently high (Table 1). This was attributed to intermittent noncompliance and unavailability of active vitamin D. The patient had also been prescribed calcium carbonate as a phosphate binder.
Questions to Consider
- What are the causes of hypocalcemia with an increased PTH concentration?
- What is the explanation for the persistently increased PTH concentrations?
- What is the role, if any, of molecular testing in a case like this?
Final Publication and Comments
The final published version with discussion and comments from the experts appears
in the February 2018 issue of Clinical Chemistry, approximately 3-4 weeks after the Student Discussion is posted.
Educational Centers
If you are associated with an educational center and would like to receive the cases and
questions 3-4 weeks in advance of publication, please email [email protected].
AACC is pleased to allow free reproduction and distribution of this Clinical Case
Study for personal or classroom discussion use. When photocopying, please make sure
the DOI and copyright notice appear on each copy.
DOI: 10.1373/clinchem.2016.269555
Copyright © 2018 American Association for Clinical Chemistry