Summary
DOI: 10.1373/clinchem.2016.261925
A 3-month-old boy was seen for routine follow-up at the pediatric nephrology outpatient clinic. He had been diagnosed as having Sotos syndrome manifesting with craniofacial dysmorphism, feeding difficulties, pulmonary artery stenosis, and atrial septal defect, as well as complex urological abnormalities.
Student Discussion
Student Discussion Document (pdf)
K.G.E. van Roij,1* H.J.R. van der Horst,2 I. Hubeek,3 J.A.E. van Wijk,1 and A. Bökenkamp1
1Departments of Pediatric Nephrology, 2Pediatric Urology, and 3Clinical Chemistry, VU University Medical Center, Amsterdam, The Netherlands.
*Address correspondence to this author at: Department of Pediatrics, VU University Medical Center, De Boelelaan 1117, NL-1081 HV, Amsterdam, The Netherlands. Fax +31-20-4444444; e-mail [email protected].
Case Description
A 3-month-old boy was seen for routine follow-up at the pediatric nephrology outpatient clinic. He had been diagnosed as having Sotos syndrome manifesting with craniofacial dysmorphism, feeding difficulties, pulmonary artery stenosis, and atrial septal defect, as well as complex urological abnormalities. He had bilateral hydronephrosis with megaureter and grade V vesicoureteral reflux to the left and grade I to the right kidney. At the age of 6 weeks, static renal scintigraphy using DMSA (99mTc-dimercaptosuccinic acid) to assess renal morphology, structure, and function had demonstrated almost symmetrical kidney function (split kidney function left 44% vs right 56%) without cortical scarring.
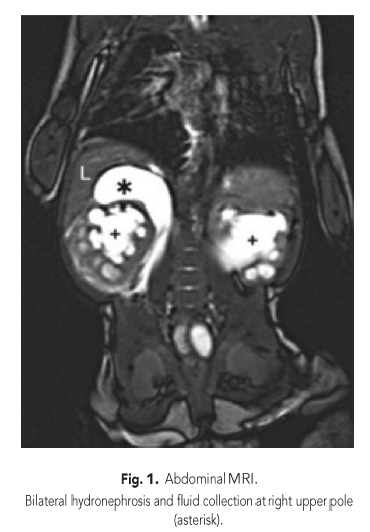
While his baseline serum creatinine had been 40 μmol/L (0.45 mg/dL), a sudden rise to 69 μmol/L (0.79 mg/dL) was noted. Urinary tract infection was ruled out, as was dehydration. On renal ultrasound, dilation of the right collecting system and ureter had increased significantly and a novel fluid collection at the upper pole was noted, which prompted an MRI study (Fig. 1). In addition to serum creatinine, cystatin C measurement was ordered and was within the reference interval for age (1.13 mg/L).
Questions to Consider
- Does the rise in creatinine indicate deterioration of kidney function?
- How do you explain the discrepancy between the 2 markers of kidney function?
- What is the nature of the fluid collection at the right upper pole?
- What test could be used to determine the nature of fluid collection?
Final Publication and Comments
The final published version with discussion and comments from the experts appears
in the April 2017 issue of Clinical Chemistry, approximately 3-4 weeks after the Student Discussion is posted.
Educational Centers
If you are associated with an educational center and would like to receive the cases and
questions 3-4 weeks in advance of publication, please email [email protected].
AACC is pleased to allow free reproduction and distribution of this Clinical Case
Study for personal or classroom discussion use. When photocopying, please make sure
the DOI and copyright notice appear on each copy.
DOI: 10.1373/clinchem.2016.261925
Copyright © 2017 American Association for Clinical Chemistry