Summary
DOI: 10.1373/clinchem.2015.244616
A previously fit and well 5-year-old girl presented to the emergency department with
right hip pain and limp following a minor fall from play equipment. X-ray imaging confirmed the
presence of a femoral fracture as well as diffuse sclerosis in the sacrum, pelvis, and bilateral
proximal femurs.
Student Discussion
Student Discussion Document (pdf)
Nilika Wijeratne,1,2,3* Kay Weng Choy,1 Zhong Xian Lu,1,2,4 Justin Brown,5,6 and James C.G. Doery1,2
1Department of Pathology and 5Monash Children’s Hospital, Monash Health, Clayton, Victoria, Australia; Departments of 2Medicine and 6Pediatrics, Monash University, Clayton, Victoria, Australia; 3Dorevitch Pathology, Heidelberg, Victoria, Australia; 4Melbourne Pathology, Collingwood, Victoria, Australia.
*Address correspondence to this author at: Dorevitch Pathology, Department of Biochemistry, 18 Banksia St. Heidelberg, Vic, 3084 Australia. Fax +61-3-9244-0207; e-mail [email protected].
Case Description
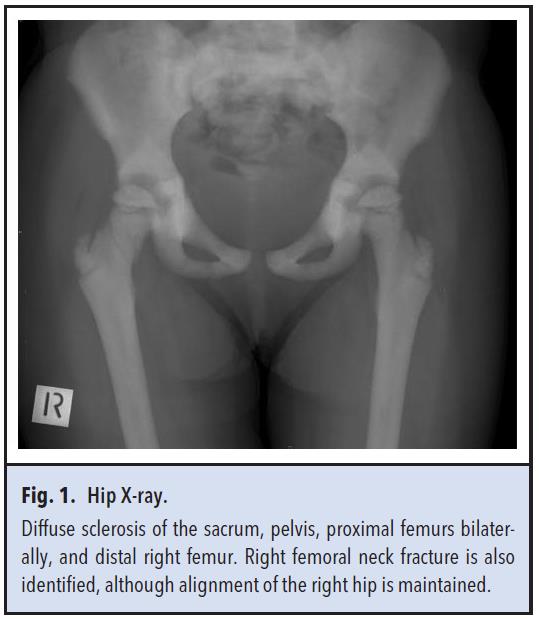
A previously fit and well 5-year-old girl presented to the emergency department with right hip pain and limp following a minor fall from play equipment. X-ray imaging confirmed the presence of a femoral fracture as well as diffuse sclerosis in the sacrum, pelvis, and bilateral proximal femurs (Fig. 1). MRI scan revealed mild stenosis of auditory canals, optic canals, and foramen magnum with no neural compression. DEXA (dual energy X-ray absorptiometry) scan showed markedly increased bone density, with a total body age-matched z score of +14. Bone marrow aspirate was normal. The patient had no other significant medical history and she was not on any regular medications. There was no family history of note but her mother also has increased bone mineral density.
Results for serum electrolytes, urea, creatinine, total calcium, phosphate, parathyroid hormone, vitamin D, alkaline phosphatase, and alanine aminotransferase were all within reference intervals. However, other biochemistry investigations revealed aspartate aminotransferase (AST) 89 U/L (reference interval, 20–80 U/L); lactate dehydrogenase (LD) 667 U/L (reference interval, 100–200 U/L); acid phosphatase (ACP) 32.1 U/L (reference interval, <6.5 U/L), with tartrate-resistant ACP 29.9 U/L (reference interval, 1.2– 4.4 U/L); creatine kinase (CK) 615 U/L (reference interval, <190 U/L); CK-MB activity by immunoinhibition technique 760 U/L (reference interval, <10 U/L); CK isoenzymes by electrophoresis, CK-MB <3% (reference interval, <6%) and CK-BB 87% (reference interval, <1%). Complete blood examination was normal except mildly low hemoglobin of 10.1 g/dL (reference interval, 11.5–15.5 g/dL).
Questions to Consider
- What conditions may cause diffuse sclerotic bone lesions?
- What is the most probable diagnosis for this girl?
- How do you explain the discrepancy between the CK-MB activity measured by the immunoinhibition method and the CK isoenzyme electrophoresis results?
Final Publication and Comments
The final published version with discussion and comments from the experts appears
in the May 2016 issue of Clinical Chemistry, approximately 3-4 weeks after the Student Discussion is posted.
Educational Centers
If you are associated with an educational center and would like to receive the cases and
questions 3-4 weeks in advance of publication, please email [email protected].
AACC is pleased to allow free reproduction and distribution of this Clinical Case
Study for personal or classroom discussion use. When photocopying, please make sure
the DOI and copyright notice appear on each copy.
DOI: 10.1373/clinchem.2015.244616
Copyright © 2016 American Association for Clinical Chemistry