Summary
DOI: 10.1373/clinchem.2015.243220
A 50-year-old woman presented with urticarial rash, fever, and pharyngitis. A week before, she had been examined in the emergency department for widespread pruritic erythematous-edematous plaques associated with remittent fever (up to 38.5 °C) and sore throat. Laboratory results revealed neutrophilic leukocytosis and increased inflammatory markers.
Student Discussion
Student Discussion Document (pdf)
Mariela Marinova,1* Mitja Nabergoj,2 Carlo Artusi,1 Martina M. Zaninotto,1 and Mario Plebani1
Departments of 1Laboratory Medicine and 2Hematology and Clinical Immunology, University-Hospital, Padova, Italy.
*Address correspondence to this author at: Department of Laboratory Medicine, University-Hospital of Padova, Via Giustiniani, 2, 135128 Padova, Italy. E-mail [email protected].
Case Description
A 50-year-old woman presented with urticarial rash, fever, and pharyngitis. A week before, she had been examined in the emergency department for widespread pruritic erythematous-edematous plaques associated with remittent fever (up to 38.5 °C) and sore throat. Laboratory results revealed neutrophilic leukocytosis and increased inflammatory markers. Thus, the woman was diagnosed with urticaria and associated mild fever, which was confirmed by a dermatologic examination. The patient had started antibiotic therapy with levofloxacin, antihistamines, and low-dose steroids. Because of the persistence of symptoms and the appearance of weakness and widespread muscle pain despite therapy, she was admitted for further assessment. At the time of admission, the patient was febrile (37.7 °C), and physical examination revealed laterocervical lymphadenopathy, hepatomegaly, and highly congested throat. Numerous confluent, erythematous, urticarial macules and papules that coalesced into urticarial plaques were observed.
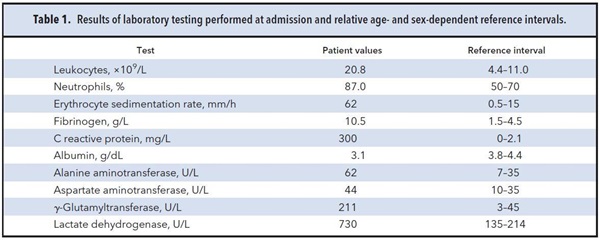
Laboratory results are shown in Table 1. Radiological examinations revealed multiple, reactive abdominal and neck lymphadenopathies of small size (maximum 15 mm).
Owing to the appearance of bilateral arthralgia of the wrists, hands, and knees, broadspectrum antibiotic therapy and low-dose methylprednisolone were started while awaiting the results of more biochemical tests. Antinuclear antibodies, extractable nuclear antigens, antineutrophil cytoplasmic antibodies, anti-dsDNA antibodies, and rheumatoid factor were negative. Complement C3 and C4 were within reference intervals. Blood and urine cultures revealed no evidence of bacterial, viral, or fungal infection. Under the suspicion of a systemic inflammatory disease, plasma ferritin was measured and found to be 20 920 µg/L (10–120 µg/L), with glycosylated ferritin 14% (50%–80%).
Questions to Consider
- What are the causes of rash and fever in adult patients?
- What are the common causes of extreme hyperferritinemia?
- What does reduced glycosylated ferritin suggest?
Final Publication and Comments
The final published version with discussion and comments from the experts appears
in the April 2016 issue of Clinical Chemistry, approximately 3-4 weeks after the Student Discussion is posted.
Educational Centers
If you are associated with an educational center and would like to receive the cases and
questions 3-4 weeks in advance of publication, please email [email protected].
AACC is pleased to allow free reproduction and distribution of this Clinical Case
Study for personal or classroom discussion use. When photocopying, please make sure
the DOI and copyright notice appear on each copy.
DOI: 10.1373/clinchem.2015.243220
Copyright © 2016 American Association for Clinical Chemistry