Summary
DOI: 10.1373/clinchem.2013.207746
A 33-year-old woman presented with amenorrhea and weight gain of 27.2–31.8 kg, despite diet and exercise, as well as progressively worsening acne. Symptoms began subsequent to a spontaneous abortion 5 years earlier and had become especially concerning during the past year. There was no notable family medical history. The patient did not report taking any prescription or over-the-counter medication and denied tobacco, alcohol, or illicit drug use. She had a blood pressure of 144/86 mmHg, heart rate of 88 beats/min, temperature of 37.1 °C, and was 1.8 m tall and weighed 105.7 kg (body mass index, 33.4). The results of a physical examination were otherwise normal.
Student Discussion
Student Discussion Document (pdf)
Tiffany K. Roberts1* and Corinne R. Fantz1
1Department of Pathology and Laboratory Medicine, Emory University, Atlanta, GA.
*Address correspondence to this author at: Tiffany K Roberts, Emory University, 1364 Clifton Rd., Rm. G163, Atlanta, GA 30322. Fax: 404-7125567; e-mail: [email protected]
Case Description
A 33-year-old woman presented with amenorrhea and weight gain of 27.2–31.8 kg, despite diet and exercise, as well as progressively worsening acne. Symptoms began subsequent to a spontaneous abortion 5 years earlier and had become especially concerning during the past year. There was no notable family medical history. The patient did not report taking any prescription or over-the-counter medication and denied tobacco, alcohol, or illicit drug use. She had a blood pressure of 144/86 mmHg, heart rate of 88 beats/min, temperature of 37.1 °C, and was 1.8 m tall and weighed 105.7 kg (body mass index, 33.4). The results of a physical examination were otherwise normal.
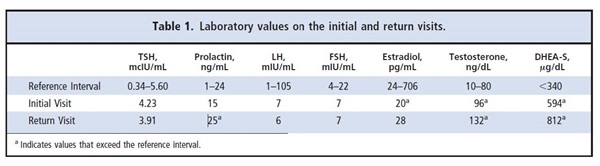
Initial laboratory evaluation results included a negative point-of-care urine human chorionic gonadotropin test and concentrations within reference intervals for thyroid stimulating hormone (TSH), prolactin, leutinizing hormone (LH), and follicle-stimulating hormone (FSH) (Table 1). Further testing revealed a low estradiol concentration (20 pg/mL, reference interval, 24–706 pg/mL), as well as increased total testosterone [96 ng/dL (DPC, Siemens, Malvern PA), reference interval, 10–80 ng/dL] and dehydroepiandrosterone-S (DHEA-S) (594 µg/dL, reference interval, 340 µg/dL) (Table 1). She was diagnosed with polycystic ovary syndrome (PCOS) and treated with metformin, which she did not tolerate, and local creams for her acne were ineffective.
Approximately 1 year later, the patient presented with continuing amenorrhea and complained of mood swings and depression as well as easy bruising and hirsutism. She was referred to an endocrinologist for further evaluation. Laboratory testing at this time included a basic metabolic panel. All measurands were within reference intervals, as were concentrations of TSH, LH, and FSH (Table 1). A random 17-hydroxyprogesterone (17OHP) was within reference intervals, and estradiol was at the lower limit of the reference interval (28 pg/mL). Prothrombin time and partial thromboplastin time were both within reference intervals. Total testosterone (132 ng/dL) and DHEA-S (812 µg/dL) remained increased.
Questions to Consider
- What is secondary amenorrhea and what are its most common causes?
- What other pathological conditions present similarly to PCOS?
- How can laboratory testing be used to diagnose the most common underlying causes of secondary amenorrhea?
- What are the possible causes of easy bruising in a patient with normal prothrombin time and partialthromboplastin time?
Final Publication and Comments
The final published version with discussion and comments from the experts appears
in the August 2014 issue of Clinical Chemistry, approximately 3-4 weeks after the Student Discussion is posted.
Educational Centers
If you are associated with an educational center and would like to receive the cases and
questions 3-4 weeks in advance of publication, please email [email protected].
AACC is pleased to allow free reproduction and distribution of this Clinical Case
Study for personal or classroom discussion use. When photocopying, please make sure
the DOI and copyright notice appear on each copy.
DOI: 10.1373/clinchem.2013.207746
Copyright © 2014 American Association for Clinical Chemistry