Summary
DOI: 10.1373/clinchem.2013.216861
A 25-year-old woman with a history of multiple medical problems including a distal pancreatectomy and splenectomy 6 months earlier for pancreatic mass (solid pseudopapillary tumor with negative margins), systemic lupus erythematous (SLE),3 Crohn disease, and a history of alcohol abuse presented to her pain management physician with weakness, decreased appetite, worsening joint pain, abdominal pain, and diarrhea (five episodes per day, some visibly bloody).
Student Discussion
Student Discussion Document (pdf)
Marion L. Snyder1 and Stacy E.F. Melanson2*
1 LabSource, Greenville, SC; 2 Department of Pathology, Brigham and Women’s Hospital, Harvard Medical School, Boston, MA.
*Address correspondence to this author at: Department of Pathology, Brigham and Women’s Hospital, Harvard Medical School, Boston, MA. Fax 617-731-4872; E-mail [email protected].
Case Description
A 25-year-old woman with a history of multiple medical problems including a distal pancreatectomy and splenectomy 6 months earlier for pancreatic mass (solid pseudopapillary tumor with negative margins), systemic lupus erythematous (SLE), Crohn disease, and a history of alcohol abuse presented to her pain management physician with weakness, decreased appetite, worsening joint pain, abdominal pain, and diarrhea (five episodes per day, some visibly bloody). At presentation, her vital signs included temperature 97.1 °F, blood pressure 127/89 mmHg, and heart rate 97 beats/min. Physical exam was remarkable for hyperactive bowel sounds, diffuse joint pain, and periumbilical pain at the surgical incision site described as constant and gnawing and graded 8 out of 10. She was prescribed morphine and oxycodone (as needed) for pain; hydroxychloroquine and prednisone for SLE; and mesalamine, docusate, and infliximab for Crohn disease.
She was referred to her gastroenterologist for management of her gastrointestinal complaints. Her dosages of prednisone and hydroxychloroquine were maintained to control her SLE. Pulse doses of steroids and a higher dose of prednisone were considered, but the risk of infection was determined to be too great. Before refilling her morphine and oxycodone prescriptions, her physician confirmed that her previous urine drug testing results showed the presence of her prescribed medications (and related metabolites), suggesting medication compliance, as well as no unexpected drugs. The physician also performed a pill count and documented her last dose of morphine (that morning) and oxycodone (3 days before). In addition, she was asked to complete a Screener and Opioid Assessment for Patients with Pain questionnaire (1), designed to assess her risk of medication noncompliance and abuse. On the basis of her responses to the questionnaire, the pill count, and her previous consistent urine drug testing results, the physician felt she was at low risk for noncompliance and renewed her oxycodone and morphine prescriptions. Because her last urine drug testing was performed 5 months earlier, he requested that she also submit a new urine sample for testing.
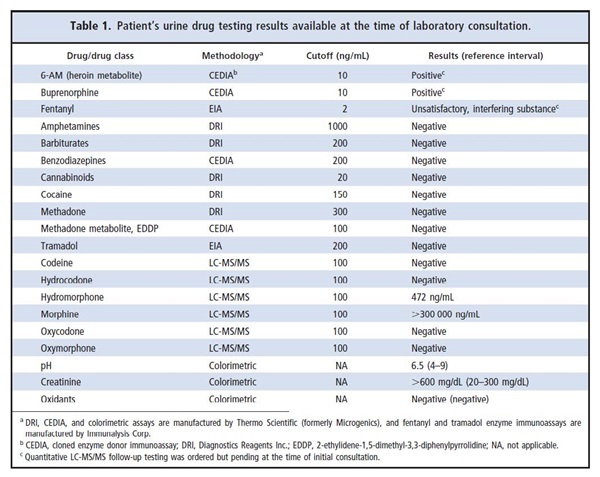
After 3 days, the physician viewed the patient’s most recent urine drug testing results, at which time only results for in-house testing were available (Table 1). The patient’s urine screened positive for 6-acetylmorphine (6-AM), a unique heroin metabolite, and buprenorphine. The fentanyl screen was unsatisfactory due to an interfering substance. All other screening results were negative. Adulterant testing was significant for a creatinine of ˃600 mg/dL in a relatively darkly colored urine. Specific opioid testing by LC-MS/MS revealed the presence of morphine (˃300 000 ng/mL) and hydromorphone (472 ng/mL). Codeine, hydrocodone, oxycodone, and oxymorphone were not detected. Reflexive tests to confirm the positive 6-AM and buprenorphine and the indeterminate fentanyl were ordered but pending. On the basis of the results available at the time, the physician was concerned that the patient might be abusing multiple undisclosed drugs, including heroin, buprenorphine, and/or fentanyl. He contacted the laboratory director for assistance in interpreting the unexpected urine drug testing results.
Referenced
- Manchikanti L, Atluri S, Trescot AM, Giordano J. Monitoring opioid adherence in chronic pain patients: tools, techniques, and utility. Pain Physician 2008;11:S155–80.
Questions to Consider
- Why is urine drug testing used to monitor patients treated with opioids for chronic pain?
- What are the limitations of immunoassays, particularly for monitoring medication compliance in patients treated for chronic pain?
- What is the significance of the patient’s urine creatinine result?
- Do this patient’s screening results indicate undisclosed heroin, buprenorphine, and/or fentanyl use?
Final Publication and Comments
The final published version with discussion and comments from the experts appears
in the December 2014 issue of Clinical Chemistry, approximately 3-4 weeks after the Student Discussion is posted.
Educational Centers
If you are associated with an educational center and would like to receive the cases and
questions 3-4 weeks in advance of publication, please email [email protected].
AACC is pleased to allow free reproduction and distribution of this Clinical Case
Study for personal or classroom discussion use. When photocopying, please make sure
the DOI and copyright notice appear on each copy.
DOI: 10.1373/clinchem.2013.216861
Copyright © 2014 American Association for Clinical Chemistry