Summary
DOI: 10.1373/clinchem.2011.163543
A 54-year-old asymptomatic man with a 5-year history of type 2 diabetes mellitus (T2DM)5 was found to have an extremely low serum cholesterol concentration. He had no history of major childhood illness, malabsorption, or any cardiovascular or neurologic dysfunction. He had smoked for 30 years and was not using alcohol or any lipid-lowering drugs. Additionally, he was not a vegetarian. His family history included stroke (father died at age 52 years) and chronic kidney disease (57-year-old brother). His eldest son had died of a suspected myocardial infarction at the age of 21 years.
Student Discussion
Student Discussion Document (pdf)
Ugur Turk,1 Gunes Basol,2* Burcu Barutcuoglu,2 Fahri Sahin,3 Sara Habif,2
Patrizia Tarugi,4 and Oya Bayindir2
1Department of Cardiology, Central Hospital, Izmir, Turkey; Departments of 2Clinical Biochemistry and 3Hematology, Ege University Faculty of Medicine, Izmir, Turkey; 4Department of Biomedical Sciences, University of Modena e Reggio Emilia, Modena, Italy.
*Address correspondence to this author at: Ege University Faculty of Medicine, Department of Clinical Biochemistry, 35100 Izmir, Turkey. Fax: 90-232-3392144; E-mail: [email protected].
Case Description
A 54-year-old asymptomatic man with a 5-year history of type 2 diabetes mellitus (T2DM) was found to have an extremely low serum cholesterol concentration. He
had no history of major childhood illness, malabsorption, or any cardiovascular or neurologic dysfunction. He had smoked for 30 years and was not using alcohol or any lipid-lowering drugs. Additionally, he was not a vegetarian. His family history included stroke (father died at age 52 years) and chronic kidney disease (57-year-old brother). His eldest son had died of a suspected myocardial infarction at the age of 21 years. The
patient had a blood pressure of 120/80 mmHg, a heart rate of 78 beats/min, and a body mass index of 32 kg/m2. The results of a physical examination were normal. Hepatic
steatosis and mild hepatomegaly were observed via abdominal ultrasonography. A transthoracic echocardiogram was normal, and the results of a treadmill exercise
test (Bruce protocol) were negative.
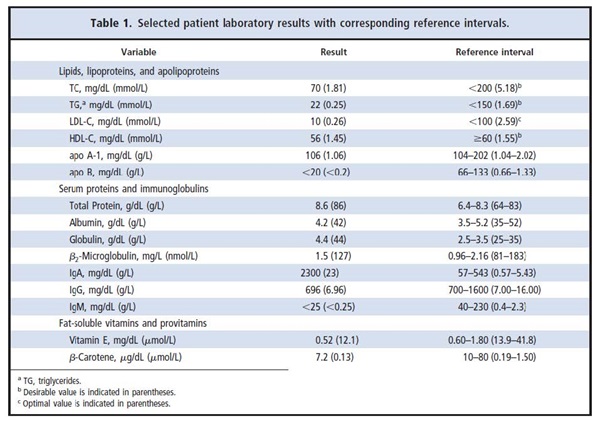
Laboratory studies were performed. Serum concentrations of liver enzymes, results of thyroid function tests, and values of hematology parameters were all normal, as were those for serum bilirubin, creatinine, urea nitrogen, uric acid, and calcium. The fasting serum glucose concentration was increased [155 mg/dL (8.6 mmol/L); reference interval, 60–110 mg/dL (3.33–6.11 mmol/L)], and the patient’s hemoglobin A1c value was 7% (reference interval, 4%–6%). The laboratory results for serum lipids, lipoproteins, apolipoproteins, proteins, immunoglobulins, and fat-soluble vitamins and provitamins are shown in Table 1. Of note, the serum concentrations of total cholesterol (TC), triglycerides, LDL cholesterol (LDL-C), and apolipoprotein B (apo B) were all markedly decreased. The serum concentrations of total protein and globulin were both high. The results of serologic tests for hepatitis A, B, and C viruses and HIV were negative.
Questions to Consider
- What are the typical lipid abnormalities seen in persons with T2DM?
- What are possible causes for low serum cholesterol, LDL, and apo B?
- What further testing could be done to clarify the cause of the decreased lipid concentrations in this case?
- Given the patient’s serum total protein and globulin results, what additional testing should be performed?
Final Publication and Comments
The final published version with discussion and comments from the experts appears
in the May 2012 issue of Clinical Chemistry, approximately 3-4 weeks after the Student Discussion is posted.
Educational Centers
If you are associated with an educational center and would like to receive the cases and
questions 3-4 weeks in advance of publication, please email [email protected].
AACC is pleased to allow free reproduction and distribution of this Clinical Case
Study for personal or classroom discussion use. When photocopying, please make sure
the DOI and copyright notice appear on each copy.
DOI: 10.1373/clinchem.2011.163543
Copyright © 2012 American Association for Clinical Chemistry