Summary
DOI: 10.1373/clinchem.2010.157248
A 34-year-old woman presented to the emergency department with a chief complaint of acutely worsening abdominal pain. The patient reported the abdominal pain to be in the left lower quadrant and of several months' duration but noted that it had worsened substantially over the previous 10 days. She also reported diffuse muscle pain and nausea without emesis, no food intake over the previous 72 h, and only limited recent fluid intake consisting of ginger ale, water, Gatorade, and homemade liquor. Her last menstrual period was 2 weeks before admission. Her medical history was remarkable for posttraumatic stress disorder, bipolar disorder, gestational diabetes, a previous gastric bypass surgery, and an ambiguous history of “injury to the liver and pancreas.” She denied taking any medications or other illicit drugs, specifically denied “binge” drinking, and had recently received a tattoo from an unlicensed tattoo artist. She was homeless and resided in a tent city with her husband.
Student Discussion
Student Discussion Document (pdf)
Peter L. Platteborze, Petrie M. Rainey, and Geoffrey S. Baird*
Department of Laboratory Medicine, University of Washington Medical Center, Seattle, WA.
* Address correspondence to this author at: Department of Laboratory Medicine, NW120, 1959 NE Pacific, Seattle, WA 98195. Fax 206-598-6189; e-mail [email protected].
Case Description
A 34-year-old woman presented to the emergency department with a chief complaint of acutely worsening abdominal pain. The patient reported the abdominal pain to be in the left lower quadrant and of several months’ duration but noted that it had worsened substantially over the previous 10 days. She also reported diffuse muscle pain and nausea without emesis, no food intake over the previous 72 h, and only limited recent fluid intake consisting of ginger ale, water, Gatorade, and homemade liquor. Her last menstrual period was 2 weeks before admission. Her medical history was remarkable for posttraumatic stress disorder, bipolar disorder, gestational diabetes, a previous gastric bypass surgery, and an ambiguous history of ―injury to the liver and pancreas. She denied taking any medications or other illicit drugs, specifically denied ―binge drinking, and had recently received a tattoo from an unlicensed tattoo artist. She was homeless and resided in a tent city with her husband.
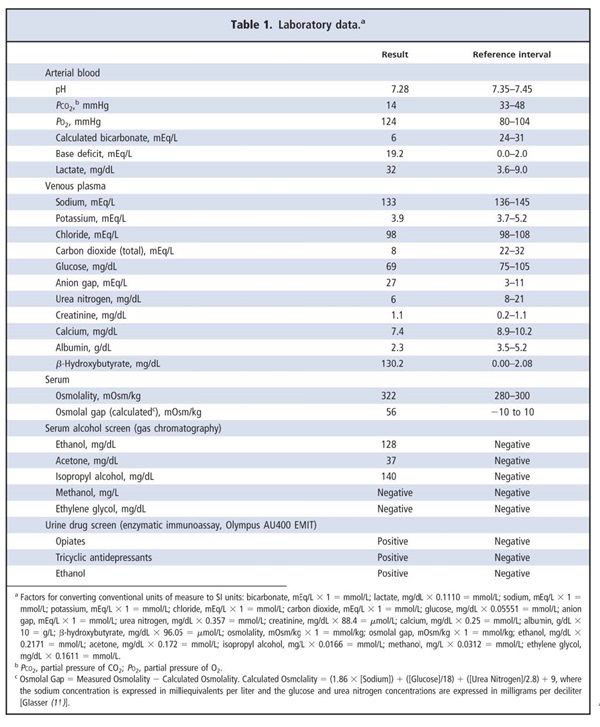
The only remarkable findings of the physical examination were tachycardia and a mildly enlarged, nontender liver. She appeared ill and smelled of a campfire but was otherwise awake, alert, and cooperative. Selected laboratory results are shown in Table 1. Low urea nitrogen and albumin concentrations suggested probable malnutrition. The observed hypocalcemia of 7.4 mg/dL could be attributed only partly to the low albumin concentration, because the albumincorrected total Ca concentration—which is equal to the measured total [Ca] + 0.8 mg/dL × (4.0 – [Albumin]), where [Ca] is the calcium concentration in milligrams per deciliter and [Albumin] is the albumin concentration in grams per deciliter (1)—was 8.8 mg/dL, less than the institutional lower reference limit.
Opiates and tricyclic antidepressants were identified in the patient’s urine. The presence of opiates was not commented on in the medical record, so whether the clinical team was aware of this finding was unknown. The records of the hospital system did not have any prescriptions for tricyclic antidepressants for the patient, so the positive result for this analyte could be due to the use of a tricyclic antidepressant obtained illicitly or with an outside prescription; alternatively, it could be due to a cross-reacting substance.
The attending physician in the emergency department requested assistance in interpreting the highly increased concentration of β-hydroxybutyrate. Furthermore, the clinical team wanted to know if detecting isopropyl alcohol in the alcohol screen implied that the homemade liquor ingested by the patient contained isopropyl alcohol.
Questions to Consider
- What are common causes of a combined high anion gap and increased osmolality?
- What can cause ketoacidosis?
- What is the appropriate approach to this patient with an increased serum isopropyl alcohol result?
Final Publication and Comments
The final published version with discussion and comments from the experts appears
in the October 2011 issue of Clinical Chemistry, approximately 3-4 weeks after the Student Discussion is posted.
Educational Centers
If you are associated with an educational center and would like to receive the cases and
questions 3-4 weeks in advance of publication, please email [email protected].
AACC is pleased to allow free reproduction and distribution of this Clinical Case
Study for personal or classroom discussion use. When photocopying, please make sure
the DOI and copyright notice appear on each copy.
DOI: 10.1373/clinchem.2010.157248
Copyright © 2011 American Association for Clinical Chemistry