Summary
DOI: 10.1373/clinchem.2011.163766
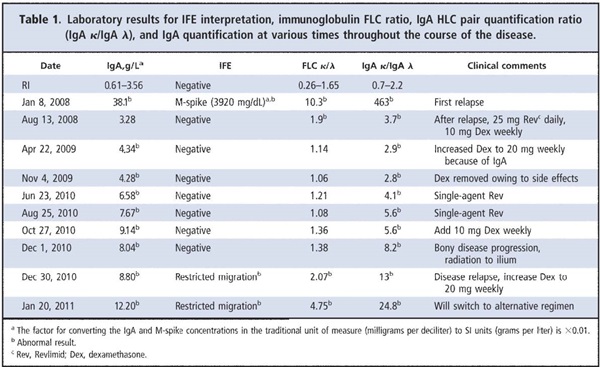
A 71-year-old woman with a 9-year history of monoclonal gammopathy of undetermined significance presented with anemia [hemoglobin, 11.6 g/dL (116 g/L); reference interval (RI),3 12–15.5 g/dL (120–155 g/L)], an increased serum calcium concentration [10.2 mg/dL (2.55 mmol/L); RI, 8.9–10.1 mg/dL (2.22–2.52 mmol/L)], and a 4800-mg/dL (48-g/L) monoclonal protein band (M-spike) after serum protein electrophoresis (SPEP). Immunofixation electrophoresis (IFE) revealed a monoclonal IgA κ protein. Her IgA concentration was markedly increased to 4720 mg/dL [47.2 g/L; RI, 61–356 mg/dL (0.61–3.56 g/L)], and the serum immunoglobulin free light chain (FLC) κ/λ ratio was 7 (RI, 0.26–1.65).
Student Discussion
Student Discussion Document (pdf)
Leslie J. Donato,1 Steven R. Zeldenrust,2 David L. Murray,1 and Jerry A. Katzmann1,2*
1Department of Laboratory Medicine and Pathology and 2Division of Hematology, Mayo Clinic, Rochester, MN.
*Address correspondence to this author at: Division of Clinical Biochemistry and Immunology, Department of Laboratory Medicine and Pathology, Mayo Clinic, 200 First St. S.W., Rochester, MN 55905. Fax 507-266-4088; e-mail [email protected].
Case Description
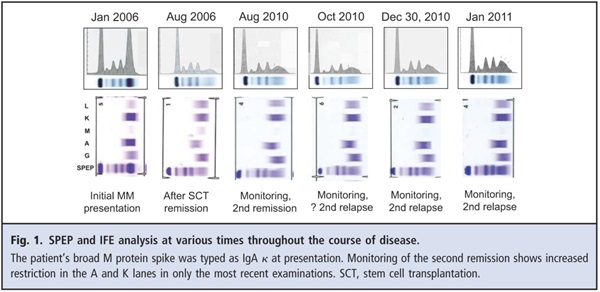
A 71-year-old woman with a 9-year history of monoclonal gammopathy of undetermined significance presented with anemia [hemoglobin, 11.6 g/dL (116 g/L); reference interval (RI), 12–15.5 g/dL (120–155 g/L)], an increased serum calcium concentration [10.2 mg/dL (2.55 mmol/L); RI, 8.9–10.1 mg/dL (2.22–2.52 mmol/L)], and a 4800 mg/dL (48 g/L) monoclonal protein band (M-spike) after serum protein electrophoresis (SPEP). Immunofixation electrophoresis (IFE) revealed a monoclonal IgA κ protein. Her IgA concentration was markedly increased to 4720 mg/dL [47.2 g/L; RI, 61–356 mg/dL (0.61–3.56 g/L)], and the serum immunoglobulin free light chain (FLC) κ/λ ratio was 7 (RI, 0.26–1.65). A bone marrow biopsy confirmed 40% involvement by monoclonal κ-restricted plasma cells with a plasma cell labeling index of 0.4% (intermediate). A bone survey revealed diffuse osteopenia, multiple small lytic lesions throughout the skeleton, and a lesion consistent with a plasmacytoma at T7. A diagnosis of multiple myeloma (MM) (Durie–Salmon stage IIIA, international stage 2) was confirmed. The patient was initially treated medically and then underwent successful autologous stem cell transplantation. The patient was asymptomatic, with negative results in serum and urine protein electrophoresis and IFE evaluations for 1.5 years.
A follow-up SPEP evaluation 2 years after the patient received her transplant revealed an M-spike of 3920 mg/dL (39.2 g/L) and an IgA concentration of 3810 mg/dL (38.1 g/L). A bone marrow biopsy showed 60%–70% involvement by monoclonal plasma cells. The results of a urine IFE test were negative. The patient was treated with a regimen of 25 mg Revlimid daily on days 1–21 and 20 mg dexamethasone weekly. The patient’s M-spike decreased to 1100 mg/dL (11 g/L) by 1 month after treatment, and her IgA concentration was reduced to 1260 mg/dL (12.6 g/L). Two months into treatment, the patient had detectable monoclonal protein but no measurable M-spike, and her IgA concentration was 402 mg/dL (4.02 g/L). The dexamethasone dosage was reduced to 10 mg weekly for the third month, and her serum IgA concentration decreased further, to 340 mg/dL (3.4 g/L), which is within the RI.
Questions to Consider
- What are the potential causes of a steadily increasing immunoglobulin in an MM patient in remission?
- What are the criteria for laboratory detection of MM relapse?
- What tests can be used to determine the clonality of serum immunoglobulins?
Final Publication and Comments
The final published version with discussion and comments from the experts appears
in the December 2011 issue of Clinical Chemistry, approximately 3-4 weeks after the Student Discussion is posted.
Educational Centers
If you are associated with an educational center and would like to receive the cases and
questions 3-4 weeks in advance of publication, please email [email protected].
AACC is pleased to allow free reproduction and distribution of this Clinical Case
Study for personal or classroom discussion use. When photocopying, please make sure
the DOI and copyright notice appear on each copy.
DOI: 10.1373/clinchem.2011.163766
Copyright © 2011 American Association for Clinical Chemistry