Summary
DOI: 10.1373/clinchem.2009.137596
A 3-year-old girl was transferred from an outside hospital to the emergency department after being found shivering and unattended outside of a public shopping area in winter. She presented with decreased mental status and possible hypothermia; she was lethargic and slipped in and out of consciousness. No cause for this alteration in her mental state was obvious; however, a physical examination revealed multiple abrasions and bruises. The patient had a temperature of 37 °C, a blood pressure of 134/74 mmHg, a heart rate of 103 beats/min, and a respiratory rate of 24 breaths/min. Computed tomography scans, a skeletal survey, and an ophthalmologic examination did not reveal additional injuries. An intravenous bolus of the opioid antagonist naloxone (Narcan) was administered shortly after her arrival in the emergency department.
Student Discussion
Student Discussion Document (pdf)
Joely A. Straseski,1 Andrew Stolbach,2 and William Clarke1*
1Department of Pathology and 2School of Medicine, Johns Hopkins Medical Institutions, Baltimore, MD.
*Address correspondence to this author at: Johns Hopkins Medical Institutions, Department of Pathology, 600 N. Wolfe St., Meyer B-125D, Baltimore, MD 21287. Fax 410-955-0767; e-mail [email protected].
3 Nonstandard abbreviations: CEDIA, cloned enzyme donor immunoassay; LCMS/MS, liquid chromatography–tandem mass spectrometry.
Case Description
A 3-year-old girl was transferred from an outside hospital to the emergency department after being found shivering and unattended outside of a public shopping area in winter. She presented with decreased mental status and possible hypothermia; she was lethargic and slipped in and out of consciousness. No cause for this alteration in her mental state was obvious; however, a physical examination revealed multiple abrasions and bruises. The patient had a temperature of 37 °C, a blood pressure of 134/74 mmHg, a heart rate of 103 beats/min, and a respiratory rate of 24 breaths/min. Computed tomography scans, a skeletal survey, and an ophthalmologic examination did not reveal additional injuries. An intravenous bolus of the opioid antagonist naloxone (Narcan) was administered shortly after her arrival in the emergency department.
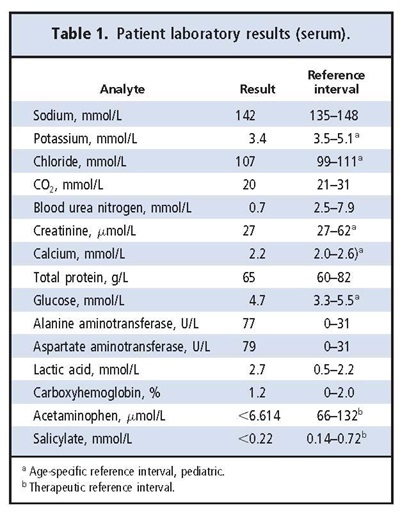
Routine hematology and chemistry tests were performed and revealed decreased serum urea nitrogen, along with increased lactate, aspartate aminotransferase, and alanine aminotransferase (Table 1). Serum acetaminophen and salicylate were not detected, and blood carboxyhemoglobin was not increased. Urine and stool cultures were negative, as was a nasal swab for methicillin-resistant Staphylococcus aureus. Toxicologic screening of a urine sample collected upon the girl’s arrival in the emergency department detected no amphetamines, barbiturates, benzodiazepines, cocaine metabolite, opiates (codeine and morphine), tetrahydrocannabinol (marijuana), or methodone. A gas chromatographic screen for volatile substances in the patient’s serum did not detect ethanol, methanol, or isopropyl alcohol but was positive for acetone. She was admitted to a pediatric floor for further monitoring.
Early the next day, clinicians requested a second urine toxicology immunoassay screen. This sample was positive for opiates at a cutoff of 300 µg/L. Confirmatory testing by GC-MS was negative for codeine, hydrocodone, oxycodone, morphine, hydromorphone, and oxymorphone (100-µg/L cutoff). A repeat immunoassay in our laboratory substantiated the original positive opiate result, and further investigation was initiated.
Questions to Consider
- What clinical situations may produce a positive result in an opiate screen?
- How can drug cross-reactivity with clinical immunoassays be confirmed?
- What situations may warrant confirmatory testing for drugs of abuse?
- What factors should be considered when testing pediatric patients for exposure to drugs of abuse?
Final Publication and Comments
The final published version with discussion and comments from the experts appears
in the August 2010 issue of Clinical Chemistry, approximately 3-4 weeks after the Student Discussion is posted.
Educational Centers
If you are associated with an educational center and would like to receive the cases and
questions 3-4 weeks in advance of publication, please email [email protected].
AACC is pleased to allow free reproduction and distribution of this Clinical Case
Study for personal or classroom discussion use. When photocopying, please make sure
the DOI and copyright notice appear on each copy.
DOI: 10.1373/clinchem.2009.137596
Copyright © 2010 American Association for Clinical Chemistry