Illicit drug abuse remains a significant problem. Drug testing in biological specimens is the most common way to prove and deter drug abuse. Urine is the most widely used matrix for drugs of abuse testing. The advantages of urine specimen include that it is well known specimen, drugs concentrate in the urine and analytically it is an easy sample to work with. However, there are many limitations of urine specimen. These limitations include a need for special specimen collection facility and narrow detection window. Other biological specimens have been explored to circumvent these problems.
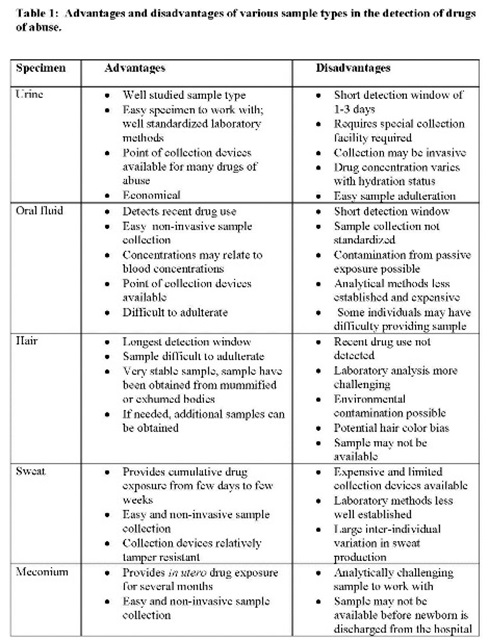
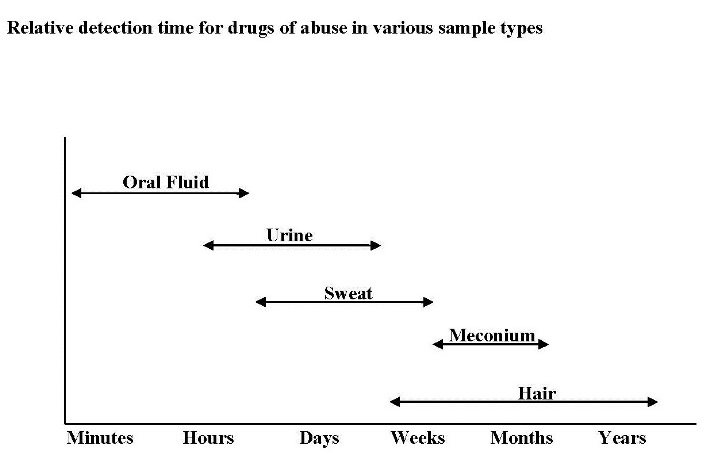
Over the years the research has shown that many other samples including hair, oral fluid, and sweat provide good alternate samples for drugs of abuse testing. Meconium has been used for detection of drug abuse during pregnancy. Most drugs of abuse including amphetamines, cocaine, cannabinoids, opiates, PCP, barbiturates, benzodiazepines, methadone, nicotine and hydroxy-butyrate, and metabolites of these drugs are detected in these specimen types. The advantages of these samples include easy sample collection without need for special sample collection facility, less intrusion during sample collection, difficult sample adulteration, longer detection window and sample stability. Advantages and disadvantages of these samples are listed in the Table, and relative drug detection periods are shown the Figure. However, the alternate samples pose many analytical and interpretative challenges. For example the drug concentrations are lower in these matrices as compared to urine, and these samples are prone to external contamination.
Most commonly used alternate sample for drugs of abuse testing is oral fluid that originates from salivary glands and drugs diffuse passively in oral fluid. Concentrations of drugs in oral fluid correlate with concentrations of free drugs in the blood. Oral fluid collection is not very well standardized. There are many commercial devices to collect oral fluid. These devices are easy to use and produce cleaner specimen than spitting. During sample collection, donor should not be allowed to have anything for 10-20 minutes before sample collection to avoid any recent oral drug exposure. Although point-of-collection devices are available, the sample is generally sent to a reference laboratory. In addition to drugs of abuse, saliva is a good specimen for alcohol testing and point of collection devices provide reliable result.
Sweat is another extensively studied specimen for drugs of abuse testing. Drugs probably enter into sweat by passive diffusion from blood to sweat glands. Usually the parent drug is present in higher concentrations in sweat than its metabolites. Sweat may be collected as liquid perspiration on sweat wipes or with a sweat patch. Sweat patch that are waterproof and tamper resistant are available commercially and can be worn comfortably for several weeks, and can provide several weeks of cumulative drug exposure.
Hair makes a good specimen for long-term exposure to drugs of abuse. Hair consists of hair follicle and hair shaft. In keratin matrix of hair, drugs are incorporated permanently in contrast to blood and urine where they are eliminated in few hours to few days. Circulating drugs or their metabolites are deposited in the hair follicles first and then get entrapped in the core of hair shaft as the hair grows out of the hair follicle. Although, specimen collection for hair analysis is not well standardized, the sample is best collected from area at the back of the head called vertex posterior. This area has less variability in hair growth and number of hairs in the growth phase, and is also less influenced by age and sex. Also, hairs in this area grow at a relatively constant rate of approximately ~0.5 inch/month. Approximately 1.5 inches long hairs that represent time period of ~90 days should be collected. Since hairs are in direct contact with the environment, they are prone to external contamination. Several approaches including thorough wash, calculating ratio of drug in the wash to the hair and use to certain cut-off, and measurement of drug metabolites have been used to circumvent issues with external contamination. Other issue with hair testing is the color of hair. Some literature suggests that dark colored hair incorporate more drugs as compared to light colored hair. At the same time there are studies that have not found higher drug positivity rate in dark hairs as compared to light color hairs.
Meconium is a useful specimen to detect drug abuse during of pregnancy. It starts forming 16-20 weeks of gestation and can detect drug use during second and third trimester. It is a thick, sticky, greenish-black newborn’s stool formed in utero. It is made of amniotic fluid, mucus, bile, and cells shed from intestinal tract, and generally passed within 24-48 h after birth. Its sensitivity in detecting intrauterine drug exposure is higher than urine. Although analytical methods are well established, meconium is a hard matrix to work with.
Overall, alternate samples provide many advantages over urine for the detection of drug abuse, and are being increasingly used and getting acceptable as specimens of choice. However, these samples pose analytical and interpretative challenges.
References:
- Garg U, Ferguson AM. Alternate specimens for drugs-of-abuse testing: preanalytical and interpretative considerations. In Clinical Toxicology Testing: A Guide for laboratory Professionals 2012. Eds M Barbarajean, MG Bissell, TC Kwong, AHB Wu, CAP Press, pp 71-80.
- Lo Muzio L, Falaschini S, Rappelli G, et al. Saliva as a diagnostic matrix for drug abuse. Int J Immunopathol Pharmacol 2005;18:567-73.
- Gambelunghe C, Rossi R, Ferranti C, Bacci M. Hair analysis by GC/MS/MS to verify abuse of drugs. J Appl Toxicol 2005;25:205-11.
- Dolan K, Rouen D, Kimber J. An overview of the use of urine, hair, sweat and saliva to detect drug use. Drug Alcohol Rev 2004;23:213-7.