
Cardiac troponin (cTn) is the key biomarker in the Universal Definition of Myocardial Infarction (UDMI) and integral to the diagnosis of myocardial infarction (MI) and myocardial injury (1). Utilization of high-sensitivity cTn (hs-cTn) assays allow for rapid triage and early diagnosis or exclusion of MI, in particular non-ST elevation MI (NSTEMI), in the Emergency Department (ED). Several hs-cTnI and hs-cTnT assays have gained approval by the Food and Drug Administration (FDA) and increasingly have been adopted and incorporated into novel algorithms and early rule-out strategies.
This article provides an overview of the analytical and clinical performance of some of the currently FDA-approved hs-cTn assays, discusses integration of hs-cTn with risk scores, and provides perspective on the future of hs-cTn assays.
DEFINITIONS, ANALYTICAL CRITERIA, AND RISK SCORES
Acute myocardial injury requires at least one troponin concentration above the 99th percentile, taken in conjunction with dynamic changes, and can occur due to multiple pathological causes. Diagnosis of acute myocardial infarction occurs if myocardial ischemia is simultaneously present based on clinical or imaging findings.
Chronic myocardial injury is characterized by increased serial hs-cTn concentrations that do not change acutely, frequently caused by long-term cardiac exposure to multiple metabolic risk factors. Chronic elevations in hs-cTn signal a poor long-term prognosis, along with increased risk for cardiovascular diseases, heart failure, and overall mortality. Large observational studies have demonstrated an association between long-term prognosis and hs-cTn concentrations even as low as the limit of blank (LoB) to the 99th percentile upper reference limit (URL).
High-sensitivity cardiac troponin assays must meet analytical criteria established by the International Federation of Clinical Chemistry and Laboratory Medicine (IFCC) Committee on Clinical Applications of Cardiac Bio-markers (C-CB) and the American Association for Clinical Chemistry (AACC) Academy, which focus on imprecision at the 99th percentile URL and the ability to measure hs-cTn in ≥50% of males and ≥50% of females above the limit of detection (LoD) within a normal healthy cohort. The recommendations for defining the reference population, along with the number of individuals required to gain statistical significance, have been recently updated by the IFCC C-CB (2).
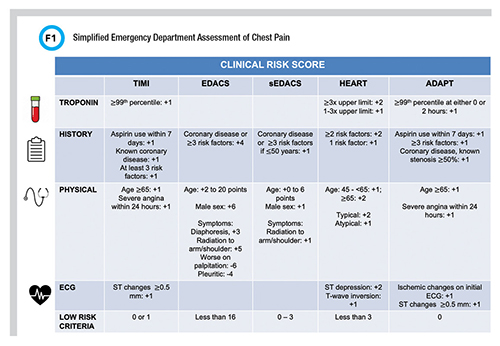
Risk scores can be utilized to identify 20−50% of patients evaluated for possible AMI who are at low risk for major adverse cardiovascular events (MACE) and may be candidates for early discharge. Commonly used risk scores include the Thrombolysis in Myocardial Infarction (TIMI); Emergency Department Assessment of Chest Pain Score (EDACS); Accelerated Diagnostic Protocol to Assess Patients With Chest Pain Symptoms Using Contemporary Troponins as the Only Biomarker (ADAPT); and the History, Electrocardiogram, Age, Risk Factors and Troponins (HEART) scores. A modified HEART score has been proposed that uses the 0/ 1-hour algorithm with high-sensitivity cardiac troponin-I assay (hs-cTnI) to identify a cohort of very low-risk chest pain patients. A simplified EDACS (sEDACS) score has also been described that uses fewer variables than in the original EDACS score (Figure 1).
ANALYTICAL PERFORMANCE CHARACTERISTICS OF HS-CTN ASSAYS
The IFCC C-CB maintains up-to-date information about the analytical characteristics of hs-cTnI and hs-cTnT assays from different manufacturers which are globally utilized (3). Further details on analytical specificity issues related to hemolysis and biotin interferences in hs-cTn assays also are published on the IFCC C-CB website. Commercially available hs-cTn assays available in the United States include those from Abbott, Beckman Coulter, Roche, and Siemens; notably, these same assays differ from ones used worldwide in that results below the limit of quantitation (LoQ) are blinded to the laboratory due to FDA restrictions.
ABBOTT HS-CTNI ASSAYS
Abbott hs-cTnI assays are approved on the ARCHITECT i1000SR, ARCHITECT i2000 and Alinity i instruments. The UTROPIA (Use of Abbott High Sensitivity Troponin I Assay in Acute Coronary Syndromes) study was a U.S.-based clinical trial that evaluated the diagnostic performance of the hs-cTnI assay on the Architect analyzer using sex-specific 99th percentiles of 16 ng/L and 34 ng/L for females and males, respectively (4).
For patients with a normal ECG and serial hs-cTnI concentrations ≤ the 99th percentile at 0 and 3 hours, the sensitivity was 100% for ruling out acute MI. For MI rule-in, the clinical specificity was 86.9% at presentation and 85.7% with serial testing, and 89.3% when a delta hs-cTnI > 5 ng/L was used. When evaluating outcomes, even individuals with measurable (from the LoD to the 99th percentile URLs) hs-cTnI within the reference interval had more than a 3-fold higher risk of MACE, including death, MI, unstable angina, revascularization, or congestive HF at 180 days compared to individuals with an undetectable hs-cTnI less than the LoD of 3 ng/L (5). Only 0.5% of patients with a baseline hs-cTnI less than the LoD had MACE at 30 days, compared to 3.0% of patients with a measurable hs-cTnI. No differences in the rate of MACE between males and females were observed. Studies in this cohort reflect the importance of interpretation of hs-cTnI concentrations as a continuous variable, as a continuum of risk.
Abbott recently received approval for hs-cTnI on the Alinity i immunoassay platform, and studies in US cohorts are expected to be forthcoming. The package insert clinical data was generated across 23 EDs from 6,174 patients presenting with symptoms consistent with acute coronary syndrome. Using sex-specific 99th percentiles (females: 14 ng/L; males: 35 ng/L), the sensitivity and negative predictive value (NPV) 0−6 hours post-presentation for females was 85.29−98.46% (NPV: 98.80−99.85%) and for males the clinical sensitivity ranged from 72.20−92.06% (NPV: 97.05−99.19%) (6).
BECKMAN COULTER HS-CTNI ASSAYS
The Beckman Coulter hs-cTnI assay received FDA-approval in 2018 for testing on the Access 2 and UniCel DxI instruments. A U.S. study evaluated the utility of the baseline hs-cTnI alone to rule out acute MI (7). While use of sex-specific cutoffs for males (20 ng/L) and females (15 ng/L) resulted in a sensitivity of 77.8% (NPV: 97.3%) and 89.5% (99.1%), respectively, even greater performance could be achieved using the LoD (<4 ng/L) for MI rule-out. Patients with a baseline hs-cTnI below the LoD had a NPV of 100.0%, sensitivity of 100% and no MACE at 30 days, effectively ruling out 40.9% of all patients presenting to the ED suspected of having acute MI.
One Australian study evaluated the diagnostic accuracy of the Beckman hs-cTnI assay in conjunction with different accelerated diagnostic pathways including EDACS, ADAPT, and HEART scores (8). The ADAPT, EDACS, and HEART pathways demonstrated high clinical sensitivity for acute MI (96.9% for ADAPT and 97.9% for EDACS and HEART), but lower sensitivity for acute coronary syndrome (≤95.0% for all). All risk scores enabled half of ED patients to be rapidly referred for objective testing and classified a significant number of patients as low risk without MACE (64.3%, 62.5%, and 49.8% for ADAPT, EDACS, and HEART, respectively).
ROCHE HS-CTNT ASSAYS
The Roche Elecsys Troponin T Gen 5 STAT is approved on the cobas e411, e601, e602, and e801 analyzers. The determined cutoffs were overall 19 ng/L, females 14 ng/L, and males 22 ng/L (9). The Rapid Evaluation of Acute Myocardial Infarction in the United States (REACTION-US) study evaluated the diagnostic performance based on results below the LoQ (6 ng/L) and a baseline/30-minute algorithm (baseline of less than 8 ng/L and 30-minute delta of less than 3 ng/L) (10). From that study, patients ruled out using the LoQ and baseline/30-minute algorithms both have an NPV of 100% and sensitivity of 100%.
Furthermore, a multisite prospective study conducted at eight U.S. sites reported improvement in NPV from 98.3% to 99% for MACE at 30 days when baseline hs-cTnT below the LoQ of 6 ng/L was used alone vs. the LoQ used in conjunction with a HEART score (11). This study reflects the importance of considering other risk factors in evaluating acute MI.
SIEMENS HS-CTNI ASSAYS
The High-Sensitivity Cardiac Troponin I in the United States (HIGH-US) study evaluated the clinical performance of the Siemens Atellica IM hs-cTnI assay using sex-specific 99th URLs derived from the AACC Universal Sample Bank (males: 53 ng/L; females: 34 ng/L). Approximately 3 hours after presentation the clinical sensitivity and specificity was >90% for all patients, with an NPV of ≥98% (12).
Furthermore, an optimized threshold of <5 ng/L safely identified 47% of all patients as low risk at presentation, resulting in a sensitivity of 98.8% and NPV of 99.7% for acute MI and a sensitivity of 98.6% and NPV of 99.6% for 30-day risk of acute MI or death (13). This study also validated specific cut points from ESC guideline recommended accelerated diagnostic protocols in this diverse US population and demonstrated a 0/1-hour or 0/2- to 3-hour algorithm could be used with acceptable performance and outcomes.
When the TIMI, HEART, and sEDACS scores were used in this cohort and supplemented with the Siemens Atellica hs-cTnI assay, the TIMI score was superior for identifying patients at risk for AMI or death within 30 days (100%). However, the sEDACS and HEART scores identified significantly more patients as low risk compared with the TIMI score (34.5%, 36.6%, and 12.1%, respectively) which allows for faster discharge from the ED without further testing (14).
The Dimension VISTA High Sensitivity TnI, EXL High-Sensitivity TnI and Advia Centaur are also Siemens hs-cTnI assays with similar clinical performance to the Atellica. However, due to lack of standardization and harmonization of hs-cTnI assays even within one manufacturer, all assays have different 99th percentiles, analytical parameters, and clinical performance.
OPPORTUNITIES IN MACHINE LEARNING AND POINT OF CARE
Several studies have demonstrated the potential utility of machine learning algorithms to provide individualized and objective assessments of the likelihood of MI to rapidly identify low- and high-risk patients for triage in the ED (15). The differences in hs-cTnI dependent on age and sex, along with variability in sampling times, can make rapid evaluation of acute MI challenging.
One study evaluated a machine learning algorithm (myocardial-ischemic-injury-index [MI3]) that incorporates age, sex, and hs-cTnI concentrations at baseline and 30 minutes in 529 patients evaluated for possible acute MI. The MI3 generates an index value from 0 to 100 reflecting the likelihood of acute MI, dividing patients into 3 categories by MI3 score: low-risk (≤3.13), intermediate-risk (>3.13−51.0), and high-risk (>51.0).
The study followed patients at 30−45 days for major adverse cardiac events (MACEs). The sensitivity for acute MI was 100% with a MI3 value ≤3.13 and 353 (67%) ruled-out after 30 minutes. At 30−45 days, there were 2 (0.6%) MACEs (2 non-cardiac deaths) in the low-risk group, in the intermediate-risk group 4 (3.0%) MACEs (3 acute MIs, 1 cardiac death), and in the high-risk group 4 (9.1%) MACEs (4 acute MIs, 2 cardiac deaths). Results of this study are promising to identify low-risk cohorts who then may be discharged earlier.
Another exciting growth area is in hs-cTn point-of-care (POC) assays. Implementing of POC testing offers the ability to expend hs-cTn across different healthcare settings and decrease the time between specimen collection and testing, ultimately expediting clinical care decisions (16).
Current requirements for hs-cTn POC assays include comparable analytical performance to the central laboratory hs-cTnI assay and that test results must be the rate-limiting step in the diagnostic pathway (17). Recent studies show promising data using the Siemens Atellica VTLi whole blood hs-cTnI assay, which satisfy the analytical criteria and with a clinical sensitivity of ≥99% for acute MI and ≥99.5% NPV (18-19). With recent advancements in hs-cTn POC technology, the future potential opportunities to integrate testing into clinical care pathways is hopefully near.
References
- Thygesen, Kristian, et al. Fourth universal definition of myocardial infarction. J Am Coll Cardiol 2018; doi: 10.1016/j.jacc.2018.08.103
- Aakre, Kristin M., et al. Analytical considerations in deriving 99th percentile upper reference limits for high-sensitivity cardiac troponin assays: Educational recommendations from the IFCC Committee on Clinical Application of Cardiac Bio-Markers. Clin Chem 2022 doi: 10.1093/clinchem/hvac092.
- International Federation of Clinical Chemistry and Laboratory Medicine. High sensitivity cardiac troponin I and T assay analytical characteristics designated by manufacturer.
https://www.ifcc.org/media/479435/high-sensitivity-cardiac-troponin-i-and-t-assay-analytical-characteristics-designated-by-manufacturer-v052022.pdf (Accessed:
June 2022).
- Sandoval, Yader, et al. Rapid rule-out of acute myocardial injury using a single high-sensitivity cardiac troponin I measurement. Clin Chem 2017; doi: 10.1373/clinchem.2016.264523
- Sandoval, Yader, et al. Clinical features and outcomes of emergency department patients with high-sensitivity cardiac troponin I concentrations within sex-specific reference intervals. Circulation 2019; doi: 10.1161/CIRCULATIONAHA.118.038284
- Abbott Laboratories. Architect STAT High Sensitivity Troponin-I https://www.corelaboratory.abbott/us/en/ (Accessed: June 2022).
- Cook, Bernard, et al. Baseline high sensitivity cardiac troponin I level below limit of quantitation rules out acute myocardial infarction in the emergency department. Crit Pathw Cardiol 2021; doi: 10.1097/HPC.0000000000000230
- Greenslade, Jaimi H., et al. Diagnostic accuracy of a new high-sensitivity troponin I assay and five accelerated diagnostic pathways for ruling out acute myocardial infarction and acute coronary syndrome. Ann Emerg Med 2018; doi: 10.1016/j.annemergmed.2017.10.030
- Fitzgerald, Robert, et al. Overall and sex-specific reference ranges for high-sensitivity troponin T Gen 5 STAT in the United States. J Am Coll Cardiol 2018; doi: doi.org/10.1016/S0735-1097(18)30774-5
- Nowak, Richard M., et al. Ultrarapid rule-out for acute myocardial infarction using the generation 5 cardiac troponin T assay: results from the REACTION-US study. Ann Emerg Med 2018; doi: 10.1016/j.annemergmed.2018.06.021
- Allen, Brandon R., et al. Diagnostic performance of high-sensitivity cardiac troponin T strategies and clinical variables in a multisite US cohort. Circulation 2021; doi: 10.1161/CIRCULATIONAHA.120.049298
- Christenson, Robert H., et al. Analytical and clinical characterization of a novel high-sensitivity cardiac troponin assay in a United States population. Clin Biochem 2020; doi: 10.1016/j.clinbiochem.2020.05.014
- Sandoval, Y and Jaffe AS. Type 2 myocardial infarction: JACC review topic of the week. J Am Coll Cardiol 2019; doi: 10.1016/j.jacc.2019.02.018
- Gibbs, Joseph, et al. The utility of risk scores when evaluating for acute myocardial infarction using high-sensitivity cardiac troponin I. Am Heart J 2020; doi: 10.1016/j.ahj.2020.05.014
- Than Martin P, et al. Machine learning to predict the likelihood of acute myocardial infarction. Circulation 2019; doi: 10.1161/CIRCULATIONAHA.119.041980
- Collet, Jean-Philippe, and Holger Thiele. Management of acute coronary syndromes in patients presenting without persistent ST-segment elevation and coexistent atrial fibrillation—Dual versus triple antithrombotic therapy. Eur Heart J 2021; doi: 10.1093/eurheartj/ehaa909
- Apple, Fred S., et al. Implementation of high-sensitivity and point-of-care cardiac troponin assays into practice: Some different thoughts. Clin Chem 2021; doi: 10.1093/clinchem/hvaa264
- Apple, Fred S., et al. Determination of sex-specific 99th percentile upper reference limits for a point of care high sensitivity cardiac troponin I assay. Clin Chem Lab Med 2021; doi: 10.1515/cclm-2021-0262
- Gunsolus, Ian L., et al. Diagnostic performance of a rapid, novel, whole blood, point of care high-sensitivity cardiac troponin I assay for myocardial infarction. Clin Biochem 2022; doi: 10.1016/j.clinbiochem.2022.04.008
Kang Xiong-Hang, PhD, is a clinical chemistry fellow at Hennepin County Medical Center in Minneapolis, Minn. +Email: [email protected]
Amy K. Saenger, PhD, DABCC, FAAC, is medical director of clinical laboratories at Hennepin County Medical Center in Minneapolis, Minn. +Email: [email protected]